


- 15 June 2026
- The Neuro-Concept Blog
The problem is no longer what we can do. It’s what we are prevented from doing.
Let’s be clear.
In neurological rehabilitation, the issue is no longer scientific.
It is not a lack of training.
It is not a lack of expertise.
👉 Today, the real problem is that the system prevents professionals from doing what they already know how to do… effectively.
Since the beginning of this series, one thing has become obvious:
We know that movement is essential 🗞️
We know that physical activity is a treatment 🗞️
We know that recovery depends on intensity, repetition, and specificity 🗞️
And above all, we know that isolated interventions are never sufficient —
👉 it is their real-time integration that drives outcomes.
In other words:
👉 we know how to treat.
So why, in clinical practice:
are patients waiting before being mobilized,
are sessions interrupted at critical moments,
are relevant tools not used when they should be?
The answer is uncomfortable, but unavoidable:
👉 because the system is structured to regulate professions… not to optimize care.
This gap between what science enables and what the system allows is no longer marginal.
It has become a direct barrier to clinical effectiveness.
At that point, one question inevitably arises:
👉 Does our current model truly protect patients…
or is it beginning to limit their chances of recovery?
A system designed to regulate… but not to adapt
The Quebec professional system is built on a fundamental principle: protection of the public. This principle is reflected in clearly defined scopes of practice, reserved acts, and regulated responsibilities.
This framework is essential.
However, in its current form, it produces a major side effect: it organizes care around professional status rather than clinical trajectories. It introduces rigidities that contradict the realities of modern rehabilitation, where patient complexity requires continuous, adaptive, and coordinated interventions.
When clinical practice exposes the system’s limitations

This gap becomes particularly visible in simple clinical situations.
Take the case of a patient in hospital neurological rehabilitation, presenting with functional deficits and requiring assisted walking. Early mobilization is a fundamental principle — it directly conditions recovery.
In practice, this mobilization depends on a prior assessment by a physiotherapist. Until this evaluation is completed, certain professionals cannot intervene, even if they have the necessary competencies.
Paradoxically, a patient attendant may walk the patient in the corridor once instructions are established, while a physical rehabilitation therapist — specifically trained in mobilization — must wait before acting.
The result is tangible: unnecessary delays, reduced intensity of mobilization, and slower patient progress than what would otherwise be achievable.
Dyspnea: fragmented intervention in real time
The same issue arises in the management of exertional dyspnea.
During a session, a patient may experience desaturation. The professional present — for example, a kinesiologist trained in cardiorespiratory rehabilitation — is able to identify the situation, adjust the exercise, and supervise the patient.
However, they cannot intervene on a key parameter: oxygen flow. This must be adjusted by an authorized professional, such as a respiratory therapist or a physiotherapist qualified to administer and titrate oxygen.
The consequence is immediate: the session is interrupted, continuity is broken, and the intervention loses its effectiveness.

Functional electrical stimulation: a recognized tool, but underused in Quebec
Functional electrical stimulation (FES) illustrates this inconsistency even more clearly.
In neurological rehabilitation, FES is widely recognized as an integrative tool used within movement to improve muscle endurance, metabolic activity, muscular activation, coordination, and functional recovery. From a scientific and clinical perspective, it is considered non-invasive in its functional applications, as it acts at the cutaneous and neuromuscular level.
In many jurisdictions — including Europe, the United States, and certain Canadian provinces such as Ontario — its use is integrated into the practice of various trained professionals, including specialized kinesiologists.
In Quebec, however, certain modalities associated with electrotherapy remain reserved activities when they involve forms of energy legally defined as invasive (any energy crossing the epidermis).
This gap between scientific recognition and regulatory framework has concrete consequences:
the professional who observes movement, adjusts the task, and accompanies the patient in real time cannot always use the tool that would immediately optimize the intervention.
The outcome is direct: either FES is not used, or the intervention becomes fragmented, or another professional must be involved to initiate and configure the FES program.
In all cases, a core principle of neurological rehabilitation is lost:
👉 the ability to act at the precise moment when motor learning is most effective.

A system based on status rather than competence
These examples converge toward the same reality: the system relies more on professional status than on actual competence.
Yet practices have evolved. Training has become more specialized. Rehabilitation professionals now develop advanced expertise that is directly relevant to real clinical situations.
Failing to allow the use of these competencies within an adapted framework artificially limits the system’s capacity to intervene.
A real impact on patients
The consequences are clear:
- reduced intervention intensity
- interrupted sessions
- lost opportunities for recovery
- fragmented care
Conversely, interdisciplinary approaches enable better coordination and more efficient use of resources.[multiresea…ournal.com]
In a context of workforce shortages, maintaining unnecessary organizational barriers becomes increasingly difficult to justify.
Rethinking patient protection
Protecting the public does not simply mean preventing errors.
It also means ensuring access to effective, coherent, and appropriate care.
Today, a fundamental question must be asked:
👉 Can an overly rigid framework, in practice, undermine that protection?
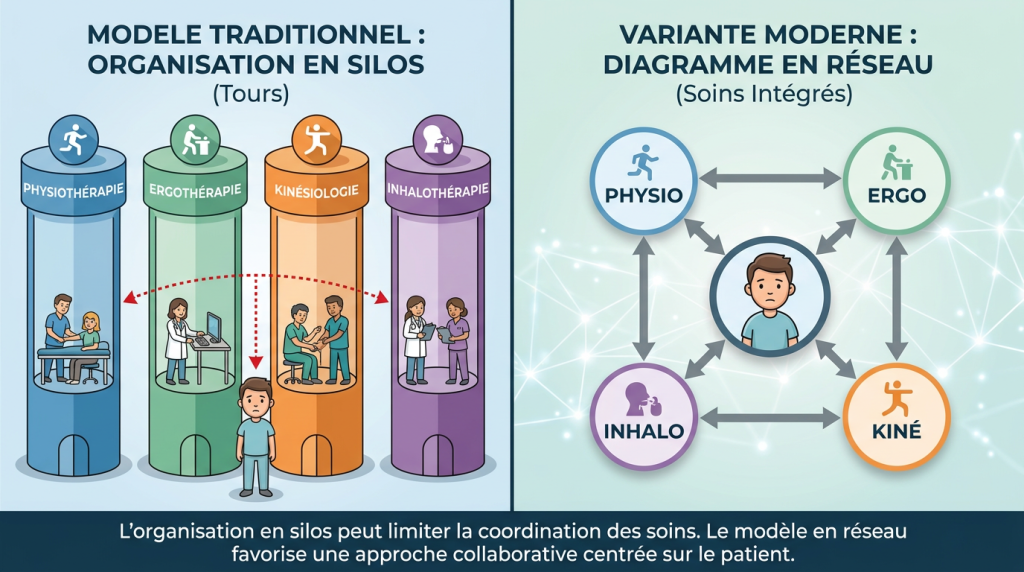
A modern healthcare system can no longer operate on a silo-based logic.
Competence must guide action.
Collaboration must replace segmentation.
And what is simple, safe, and effective in practice should never become complex because of the system.
Models That Demonstrate an Alternative Organizational Approach Is Possible
Some organizations, particularly outside the public system, have already evolved toward models centered on patient trajectories rather than professional status. These environments enable a more fluid integration of interventions and allow competencies to be mobilized precisely when they are needed.
These approaches do not compromise patient safety — on the contrary, they demonstrate that it is possible to maintain a rigorous framework while enabling more continuous, coherent, and effective interventions. They highlight that the limitations currently observed are not solely related to patients or professionals, but rather to how the system itself is structured.

Concrete avenues for evolution
Solutions exist. They rely on a structured evolution of the current model — without compromising safety:
- recognizing certain practices based on demonstrated competencies rather than solely on professional status
- developing interprofessional protocols enabling shared and supervised interventions
- reclassifying low-risk activities to facilitate access
- formalizing clinical delegation and clarifying responsibilities
- organizing care around patient trajectories rather than professional silos
👉 The issue is not deregulation.
👉 The issue is aligning the regulatory framework with clinical reality.
Références
Kongkar, R., Ruksakulpiwat, S., Phianhasin, L., et al. (2025). The impact of interdisciplinary team-based care on the care and outcomes of chronically ill patients: A systematic review. Journal of Multidisciplinary Healthcare, 18, 445–457.
Wei, H., Horns, P., Sears, S. F., et al. (2022). A systematic meta-review of systematic reviews about interprofessional collaboration: Facilitators, barriers, and outcomes. Journal of Interprofessional Care, 36(5), 735–749.
Sama, N., Yusuf, I., Aras, I., et al. (2026). Facilitators and barriers to effective interprofessional collaboration in rehabilitation services: A systematic review. Journal of Interprofessional Care.
Espat, N. N., Kumar, S., Rhodes-Lyons, H. X., & Elkbuli, A. (2025). Enhancing healthcare outcomes through interprofessional collaboration: Challenges and future directions. The American Journal of Surgery.