

- 23 June 2026
- The Neuro-Concept Blog
1. Causes of Cerebellar Ataxia
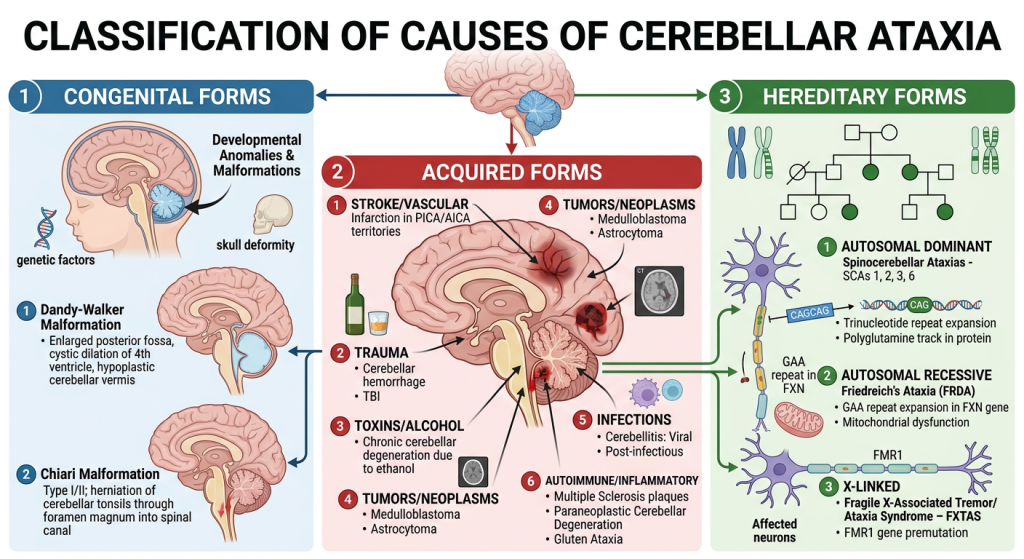
Cerebellar ataxia encompasses a group of neurological syndromes characterized by impaired motor coordination resulting from damage to the cerebellum or its connections. Its marked clinical heterogeneity is explained by the diversity of its etiologies, classically divided into hereditary, acquired, and congenital forms.
1.1 Hereditary Ataxias: Genetic Diversity and Epidemiological Features
Hereditary ataxias constitute a highly heterogeneous group of genetic disorders, including autosomal dominant spinocerebellar ataxias and autosomal recessive ataxias such as Friedreich’s ataxia. More than forty genetic forms have been identified, illustrating the complexity of these conditions. Their overall prevalence is low, generally estimated at between 1 in 33,000 and 1 in 50,000 individuals for spinocerebellar ataxias.
However, certain populations exhibit higher prevalence rates due to founder effects. Quebec provides a particularly well-documented example. A study conducted in the eastern part of the province estimated the minimum prevalence of adult hereditary ataxias at 6.47 cases per 100,000 inhabitants, a rate higher than some international estimates. This specificity is linked to genetic phenomena unique to certain regions, which have led to a concentration of specific mutations within the population. Certain forms, such as Friedreich’s ataxia and some spinocerebellar ataxias, are therefore more common in this context.
1.2 Acquired Ataxias: Neurological, Toxic, and Deficiency-Related Causes
1.3 Congenital Ataxias
2. Conceptual Advances and Multidisciplinary Management of Cerebellar Ataxia
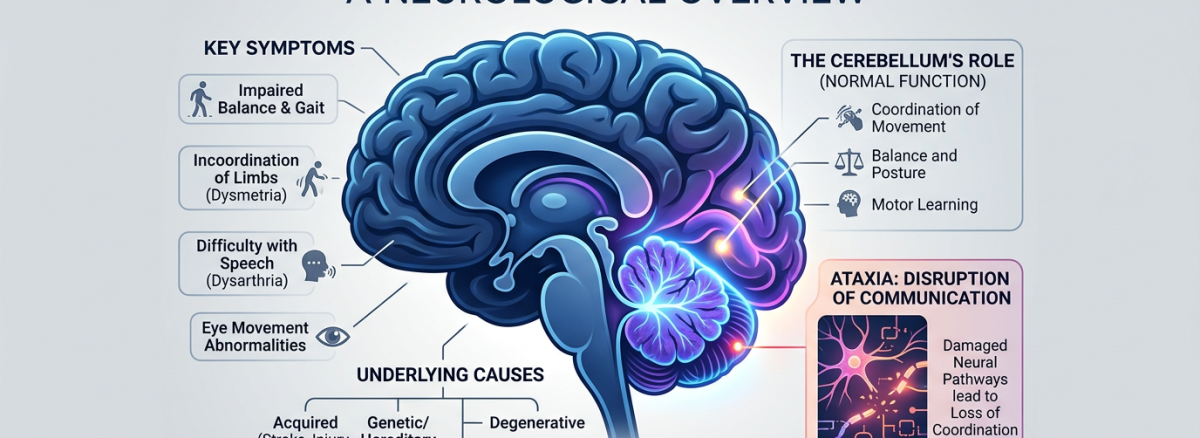
Recent advances in neuroscience have significantly reshaped our understanding of cerebellar ataxia. The cerebellum is now recognized as being involved not only in motor control but also in cognitive and emotional processes. The cerebellar cognitive-affective syndrome highlights executive dysfunction, language impairments, and emotional dysregulation in affected patients. These findings are consistent with neuroimaging observations showing close interactions between the cerebellum, the prefrontal cortex, and limbic structures.
Clinically, cerebellar ataxia manifests as a combination of motor disturbances—gait instability, dysmetria, intention tremor, and dysarthria—and cognitive and emotional impairments that contribute significantly to overall disability. This complexity requires a comprehensive assessment approach.
Management relies on coordinated multidisciplinary care. The neurologist is responsible for diagnosis, follow-up, and therapeutic orientation, particularly with the help of modern genetic technologies, whose diagnostic yield is around 40–45%.
Physiotherapy specifically targets rehabilitation of neurological motor deficits, whereas kinesiology focuses on optimizing and maintaining movement in daily life, with an emphasis on physical activity and endurance. Occupational therapy promotes functional independence through adaptation of activities and the environment, while psychological support addresses emotional and cognitive aspects.
By leveraging neuroplasticity mechanisms, multidisciplinary programs have demonstrated effectiveness. A meta-analysis showed a significant improvement in motor performance, with an average reduction of approximately 1.41 points on the SARA scale following intervention. Improvements in balance and autonomy have also been observed using functional scales such as the Berg Balance Scale and the Functional Independence Measure.
Technologies play an increasingly important role in this management. Virtual reality, exergames, and telerehabilitation help intensify interventions, improve patient engagement, and facilitate remote follow-up, thereby optimizing functional outcomes.
3. Research, Therapeutic Innovations, and Future Perspectives
At the same time, therapeutic innovations are emerging, including targeted pharmacological treatments, gene therapies, and molecular approaches aimed at modifying disease progression. Rehabilitation technologies, such as robotics and virtual reality, also help optimize interventions and collect objective data.
The integration of clinical, genetic, and radiological data into digital systems supports the development of personalized medicine. This approach allows interventions to be tailored to each patient’s profile and improves clinical outcomes while offering promising perspectives for the future.
4. Practical Aspects and Impact on Daily Life
Cerebellar ataxia has significant effects on daily life, particularly due to balance, coordination, and communication disorders. These impairments increase the risk of falls, limit independence, and may lead to social isolation.
Management aims to maintain independence and quality of life through the use of assistive devices, environmental adaptations, and the integration of supervised physical activities. Digital technologies facilitate monitoring and continuity of care, particularly in geographically dispersed settings.
References
- Matsugi A. et al. Effects of physiotherapy on degenerative cerebellar ataxia: a systematic review and meta-analysis. Frontiers in Neurology, 2025. [link.springer.com]
- Chien H.F. et al. Rehabilitation in patients with cerebellar ataxias. Arq Neuropsiquiatr, 2022. [gimopen.org]
- Alshimemeri S. et al. Demographics and clinical characteristics of spinocerebellar ataxia in Canada. Mov Disord Clin Pract, 2023. [pmc.ncbi.nlm.nih.gov]
- Haj Salem I. et al. Epidemiological study of hereditary ataxia in Eastern Quebec. CJNS, 2021. [nature.com]
- Schmahmann J.D., Sherman J.C. The cerebellar cognitive affective syndrome. Brain, 1998. [dumas.ccsd.cnrs.fr]
- Rudolph S. et al. Cognitive-affective functions of the cerebellum. Journal of Neuroscience, 2023. [link.springer.com]
- Tenorio R.B. et al. Diagnostic yield of next-generation sequencing in hereditary ataxia. Cerebellum, 2023. [frontiersin.org]
- Öz G. et al. MRI and spectroscopy in degenerative ataxias. Curr Opin Neurol, 2020. [mcgill.ca]