


- 30 June 2026
- The Neuro-Concept Blog
Silent Stroke: The Cerebrovascular Warning Signal Not to Ignore
Definition and Nosological Framework
Epidemiology
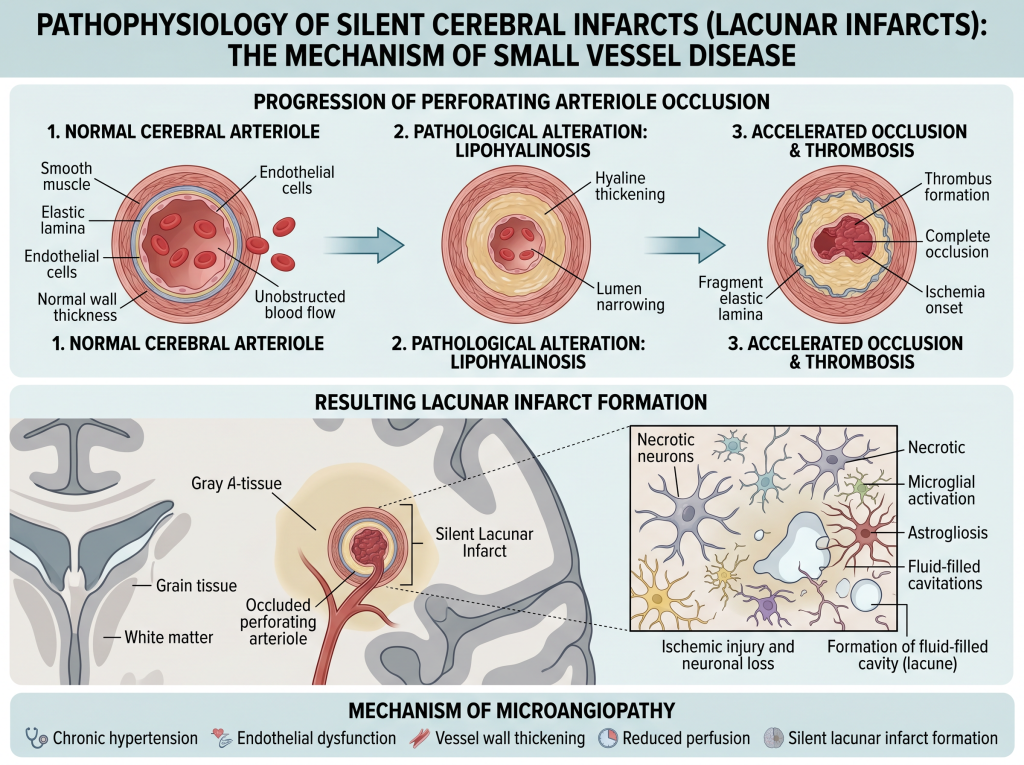
Pathophysiology
The underlying mechanisms are dominated by cerebral small vessel disease, including:
- Lipohyalinosis associated with hypertension
- Intracranial atherosclerosis
- Silent emboli (particularly in atrial fibrillation)
- Endothelial dysfunction
Lacunar infarcts (< 15 mm) result from occlusion of deep perforating arterioles.
Clinical and Prognostic Significance
Despite their initial asymptomatic nature, silent cerebral infarctions carry important implications:
Stroke Risk
The presence of SCI significantly increases the risk of symptomatic stroke, with a 2- to 4-fold increase.
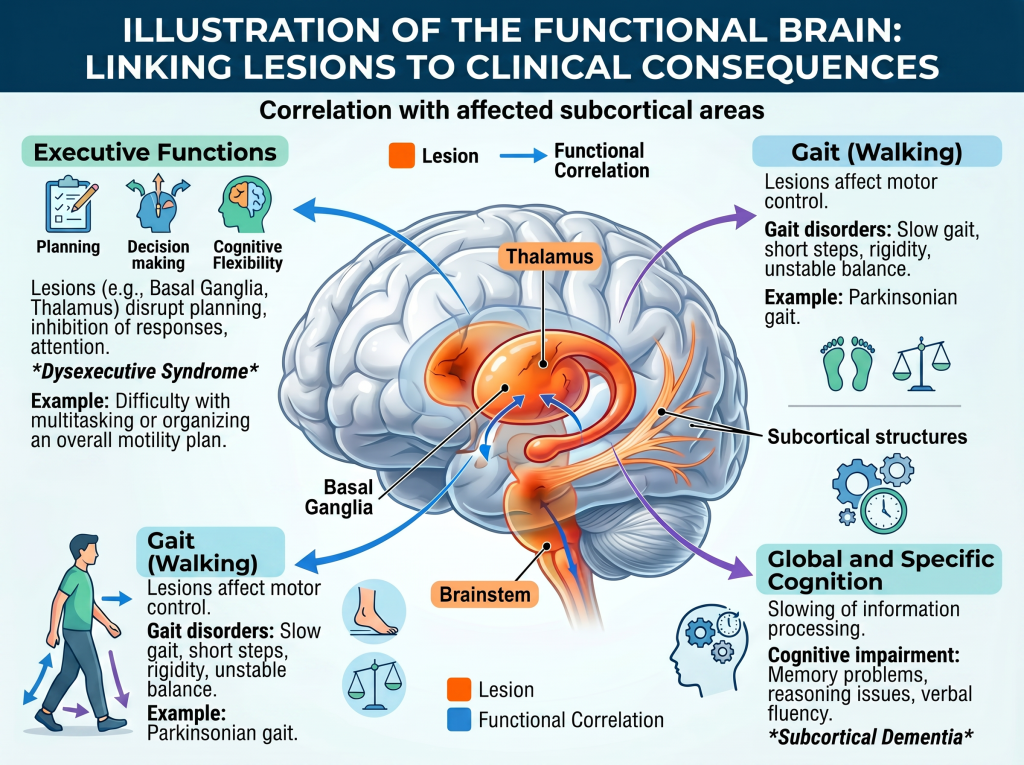
Cognitive Decline
They are associated with reduced cognitive performance and a more than twofold increased risk of dementia.
Functional Impact
Subtle disturbances in gait and balance may also occur.
Diagnosis
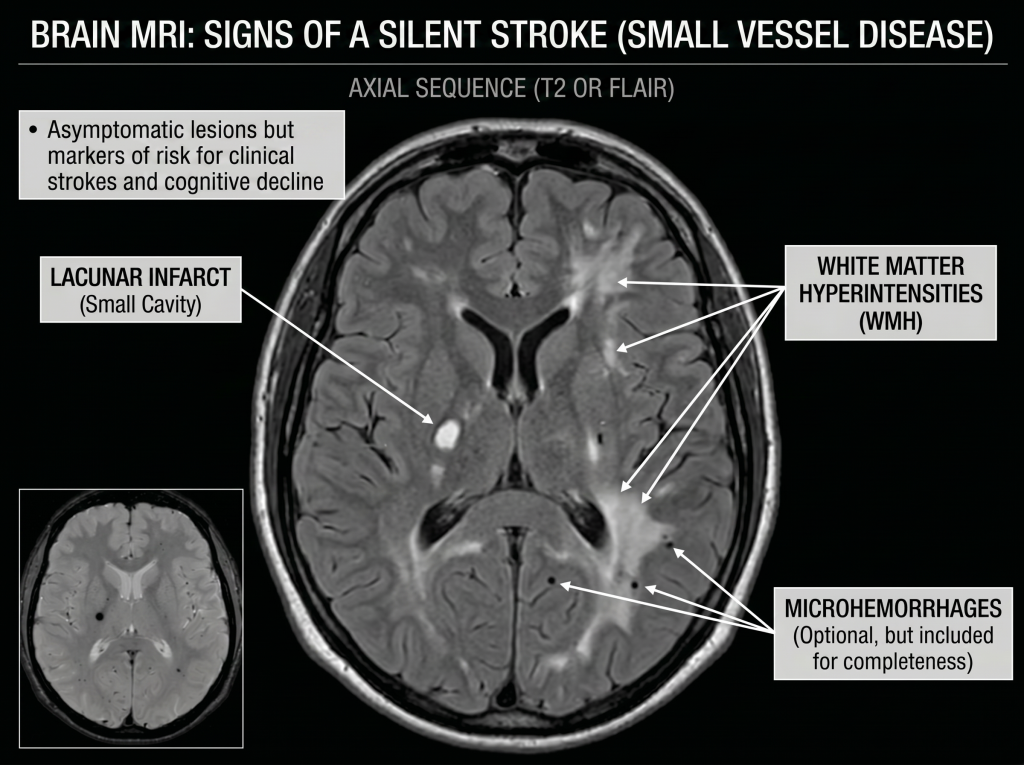
MRI is the cornerstone of diagnosis, allowing identification of:
- Lacunar infarcts
- White matter abnormalities
- Cerebral microbleeds
These lesions are usually discovered incidentally during investigations for other reasons.
Therapeutic Approach
Risk Reclassification
The presence of SCI should be interpreted as a marker of high cerebrovascular risk. Current recommendations suggest adopting an active prevention strategy similar to that used in high cardiovascular risk patients.
Control of Risk Factors
Controlling modifiable risk factors is central to management:
- Hypertension: the main contributing factor; requires strict control to limit progression of small vessel disease
- Dyslipidemia: statin therapy depending on overall risk profile
- Diabetes: optimization of glycemic control
- Smoking: complete cessation recommended
Lifestyle measures—including regular physical activity and a balanced diet—contribute to overall vascular risk reduction.
Antithrombotic Therapy
The use of antithrombotic treatments should be individualized:
- Antiplatelet agents are not systematic in the absence of a clear indication
- Anticoagulation is indicated only if a documented cardioembolic source is present (notably atrial fibrillation)
Etiological Workup
A targeted evaluation is recommended to identify a potentially treatable cause:
- Screening for atrial fibrillation (ECG, monitoring)
- Vascular assessment (carotid atherosclerosis)
- Global cardiovascular evaluation
Given the increased risk of cognitive decline:
- Initial screening (e.g., MoCA) is recommended
- Longitudinal follow-up may be considered in at-risk patients
Non-Pharmacological Interventions
Physical activity and multidisciplinary management play an important role in secondary prevention, particularly to:
- Improve cerebral perfusion
- Maintain cognitive and motor functions
- Slow progression of small vessel disease
| Step | Intervention |
|---|---|
| MRI finding | Confirm SCI |
| Evaluation | Risk factors + cardiac workup |
| Treatment | Hypertension, lipids, diabetes |
| Antithrombotic | Individualized |
| Follow-up | Cognitive + clinical |
Conclusion
Silent stroke is a frequent and clinically meaningful manifestation of cerebrovascular disease. It represents an independent risk factor for symptomatic stroke, cognitive decline, and dementia.
Its detection should prompt proactive management focused on prevention, including optimization of risk factors and appropriate clinical monitoring. In the context of population aging, it constitutes a major lever for reducing the burden of neurological and cardiovascular diseases.
References
- Vermeer SE et al. Silent brain infarcts: a systematic review. Lancet Neurology, 2007. [thelancet.com]
- Smith EE et al. Prevention of stroke in patients with silent cerebrovascular disease. Stroke, 2017. [ahajournals.org]
- Vermeer SE et al. Silent brain infarcts and risk of dementia. N Engl J Med, 2003. [nejm.org]
- Lei C et al. Silent brain infarcts and cognitive function. J Stroke Cerebrovasc Dis, 2019. [strokejournal.org]
- Caplan LR. Lacunar infarction and small vessel disease. J Stroke, 2015. [pmc.ncbi.nlm.nih.gov]
- Meinel TR et al. Management of covert brain infarction. Eur Stroke J, 2023. [pmc.ncbi.nlm.nih.gov]
- Yaghi S et al. Lacunar stroke: mechanisms and therapeutic implications. JNNP. [jnnp.bmj.com]